

2025-03-31 14:59:04
I once heard an incredible report about an auntie Liu from Zhejiang. Twenty years ago, her right foot was crushed by a car, leaving a wound that never fully healed. The injury remained inflamed, but Auntie Liu, being carefree, simply kept changing the dressings and never paid much attention to it.
In the blink of an eye, twenty years passed, yet the wound remained—now transformed into an egg-sized, fleshy mass covered with granulation tissue. Eventually, Auntie Liu’s children took her to the hospital, where the diagnosis revealed 'squamous cell carcinoma of the right heel,' a type of cancer.

What is the relationship between inflammation and cancer?
Inflammation is actually a self-protection mechanism of the body. Through inflammatory responses, the human body can prevent the spread of infection, remove necrotic tissue, and assist in organ recovery.

Prof. Rudolf Virchow (http://ihm.nlm.nih.gov/images/B25666 [Public domain])
The quote, "Cancer is a wound that does not heal, originating in inflammation," is attributed to Rudolf Virchow, the father of pathology. In 1863, he observed the presence of inflammatory cells within tumors and hypothesized that cellular proliferation at sites of injury in the human body would increase, with inflammatory cells gathering at wound sites to deal with "foreign bodies." It is precisely this continuous proliferation of cells and the constant replication and division of genetic material that leads to an increased incidence of cancer.
Long-term inflammation leading to cancer may seem like an abstract concept, but it actually has a close relationship with every one of us, ordinary people.

Firstly, people are no strangers to inflammations such as enteritis, gastritis, and appendicitis. With the increasingly fast pace of modern life and the growing mental pressure, irregular eating habits have become common. Coupled with the habits formed to relieve stress, such as smoking, drinking, staying up late, and having a preference for spicy food, it can be said that more or less everyone is troubled by these inflammations to some extent.
The factors that contribute to chronic inflammatory diseases include unreasonable dietary intake, exposure to environmental toxins, disruption of biological rhythms, and mental stress.
At the same time, people do not pay enough attention to these chronic inflammations, allowing them to lurk silently in the body and damage our health over time. During the repeated process of the body's self-repair, a large number of cells continuously proliferate and divide. The increase in the number of divisions also elevates the chance of errors in DNA replication, further increasing the incidence of chronic inflammation-related cancers.
Chronic inflammatory diseases are most commonly seen in the digestive system, and the following chronic digestive diseases are particularly closely related to cancer, warranting prompt intervention.
The carcinogenic process of chronic ulcerative colitis typically progresses as follows:
chronic ulcerative colitis → colorectal polyps or adenomas → colorectal cancer.
The carcinogenic process from superficial gastritis to gastric cancer typically progresses as follows:
superficial gastritis → atrophic gastritis → intestinal metaplasia and dysplasia → gastric cancer.
The carcinogenic process of non-alcoholic fatty liver disease typically progresses as follows:
non-alcoholic fatty liver disease → chronic hepatitis → cirrhosis → liver cancer.
Chronic ulcerative colitis and gastritis are certainly not unfamiliar to everyone, as many people have experienced these conditions to some extent. Due to the significant pain associated with the onset of colitis and gastritis, regular and timely check-ups can help in effectively controlling and treating these conditions.
But today, I want to talk about a stealthy killer—hepatitis.
During our graduation year, all four of us in the dormitory went for a pre-employment physical examination. Three of us were diagnosed with fatty liver disease, and ironically, I, the heaviest person in the dormitory, was the only one who didn't have it.

From the sentence "During our graduation year, all four of us in the dormitory went for a pre-employment physical examination. Three of us were diagnosed with fatty liver disease, and ironically, I, the heaviest person in the dormitory, was the only one who didn't have it," we can see that liver problems are often difficult to detect and can be a stealthy killer. Nonalcoholic fatty liver disease (NAFLD/NAFL) also has a high prevalence among people who may not appear to be overweight.
Non-alcoholic fatty liver disease (NAFLD) can gradually progress to hepatitis, and its development process and proportions are as follows: 10-40% of NAFLD cases can lead to non-alcoholic steatohepatitis (NASH), 50% of NASH cases can result in liver fibrosis, 15-30% of liver fibrosis cases can progress to cirrhosis, and 30-40% of cirrhosis cases can lead to liver cancer.
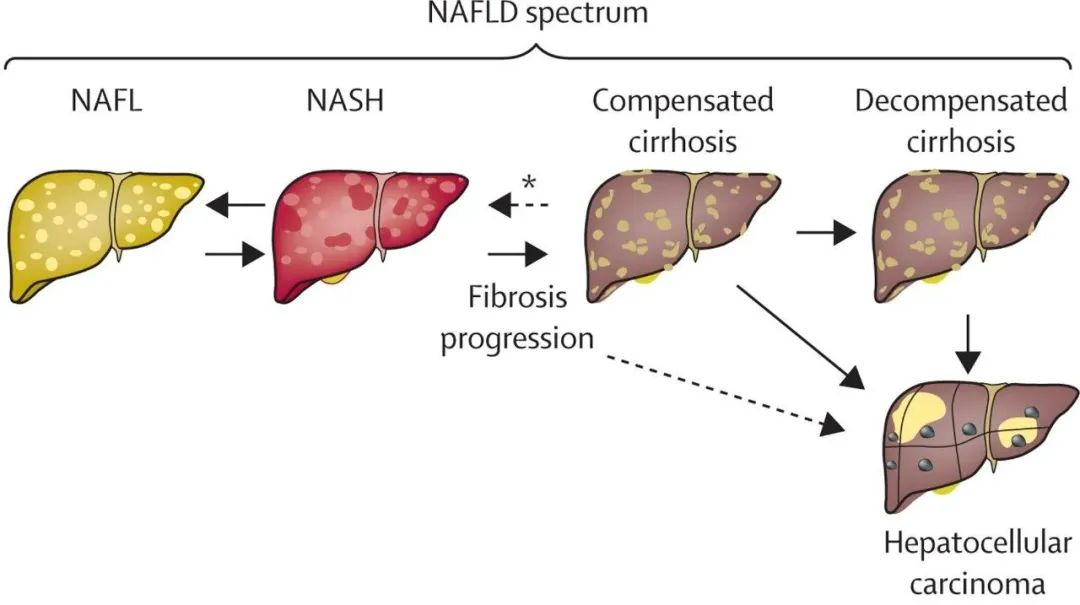
The progression from nonalcoholic fatty liver disease to liver cancer
The natural progression of NAFLD is reversible, with bidirectional changes possible across the three disease stages from nonalcoholic fatty liver (NAFL) to nonalcoholic steatohepatitis (NASH) to compensated cirrhosis, as well as in the degree of fibrosis progression. However, fibrosis, particularly advanced fibrosis (stages 3-4), serves as a critical prognostic indicator for the worsening of liver-related outcomes and increased overall mortality. A meta-analysis involving 4,428 NAFLD patients showed that patients with stage 4 fibrosis (cirrhosis) had an all-cause mortality rate 3.42 times higher and a liver-related mortality rate 11.13 times higher than those without fibrosis.
From fatty liver to hepatitis to hepatocellular carcinoma (HCC):
Excess fat → Chronic inflammation → Secretion of inflammatory cytokines → Stimulation of oncogenic signals → Occurrence of HCC.
Excess energy stored in adipose tissue can promote the production of chronic inflammation in obese individuals. Inflammatory cytokines secreted by adipocytes and macrophages, such as tumor necrosis factor (TNFα), interleukin-1 (IL-1), and interleukin-6 (IL-6), are upregulated in obesity. TNFα and IL-6 activate the JAK/STAT3 oncogenic signal in non-adipose tissues, leading to uncontrolled hepatocyte proliferation and apoptosis, which promotes the occurrence of HCC.
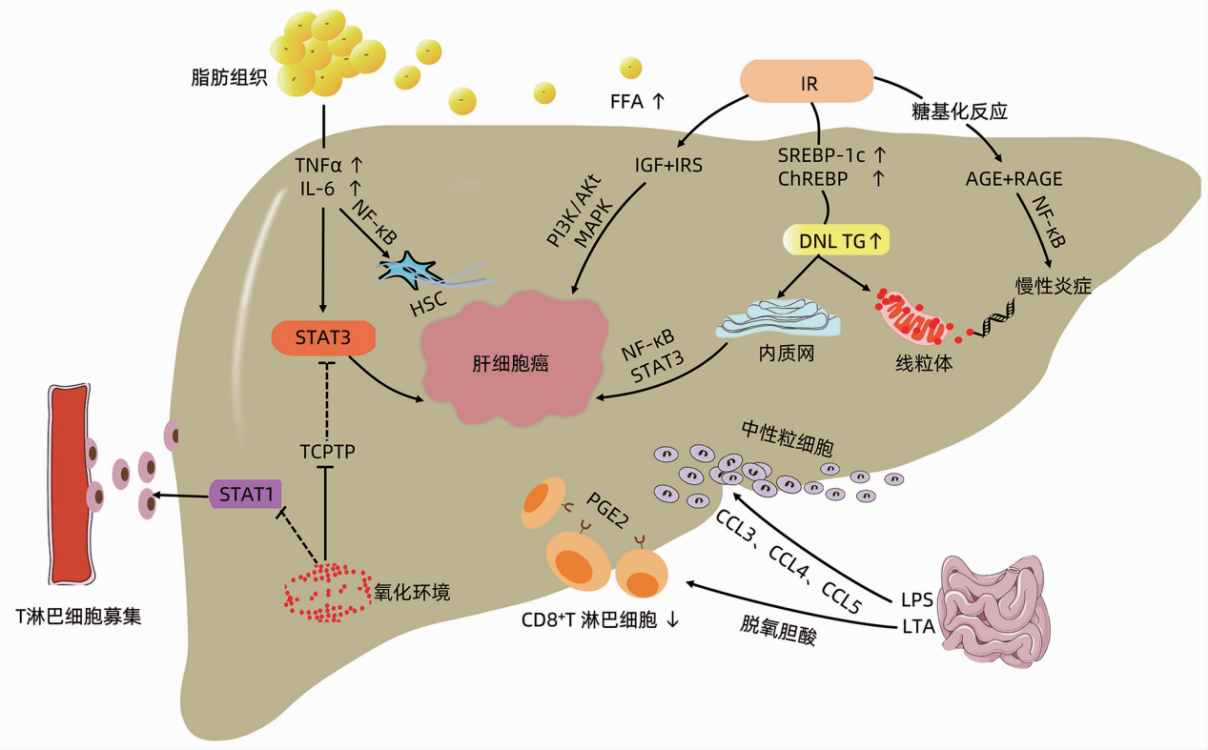 The pathogenesis of HCC related to NAFLD involves multiple complex factors and interactions. Here's a detailed overview
The pathogenesis of HCC related to NAFLD involves multiple complex factors and interactions. Here's a detailed overview
In light of hepatitis, a stealthy and terrifying carcinogen, we offer some advice on preventing fatty liver disease. Here are four tips to help you correct your dietary habits and prevent fatty liver:
Adjust Your Dietary Structure
Increase your intake of foods rich in plant fiber, with meat as a secondary choice. Additionally, enhance your consumption of vitamins and minerals. For instance, consume coarse grains, eggs, and green leafy vegetables rich in vitamin B; fresh vegetables and fruits abundant in vitamin C. Also, ensure your daily sodium intake is below 6 grams.
Develop Healthy Eating Habits
Eat three meals a day at regular times and in appropriate portions to avoid overeating. Reduce your intake of cold and spicy foods. Correct habits such as having excessive late-night snacks, consuming too much sugar, and drinking beverages instead of water to prevent excess calorie intake.
Engage in Moderate Exercise
It is recommended to engage in moderate-intensity exercise for about 60 minutes, 3-5 times a week. Activities such as jogging, dancing, aerobics, cycling uphill, skating, playing volleyball, and hiking can effectively reduce fat deposition in the liver and significantly lower the risk of nonalcoholic fatty liver disease.
Avoid Smoking and Drinking
Quitting smoking and abstaining or reducing alcohol consumption are the most effective methods for preventing nonalcoholic fatty liver disease.
Foods that are beneficial in managing fatty liver disease include soy products, goji berries, hawthorn, green tea, carrots, white fungus, garlic, tomatoes, oats, and onions.
Gu Xuelian,Li Junfeng,Mao Xiaorong. Research Progress on Hepatocellular Carcinoma Related to Nonalcoholic Fatty Liver Disease [J]. Journal of Clinical Hepatology and Gallbladder Diseases, 2022, 38(1): 196-200.
Elizabeth E Powell, Vincent Wai-Sun Wong, Mary Rinella. Non-alcoholic fatty liver disease[J]. Lancet, 2021, 397: 2212-24.
